When I started this site I had no idea that WordPress sites were such a target of spam. All bot driven, the spam is just a waste of space and time. It hurts interested commenters.
I am happy to report that I have gotten the site updated and have implemented a sophisticated spam blacker. Comments are now possible from anyone. They will be available immediately, unless you are a spammer
Possibly you might get blocked inadvertently. I apologize in advance. If this happens please email me at sholland at napervillegi dot com. There may be some additional adjustments I need to make.
I am at the AIBD conference in Orlando. This is probably the premiere clinical practice conference in the US. No chance getting to Disney World, there is just too much conference to go to!
This will be a combo blog as well as some various thoughts driven by the conference.
At the moment (1:30 on Thursday 12/12/19) I’m at an interesting conference about patient stratification for IBD. The message here (by Corey Siegel, MD) is that some patients are at high risk for severe disease. In Crohn’s, Small bowel disease, perinatal disease, ASCA level, CBir1 level, and presence of NOD 2 mutation predict more severe disease. Using systems dynamics Analysis suggests whether a patient should consider getting biological therapy early in their disease course to prevent anticipated complications. This analysis gives a predicted course of progress of the illness and informs choices for early use of or not needing biologics.
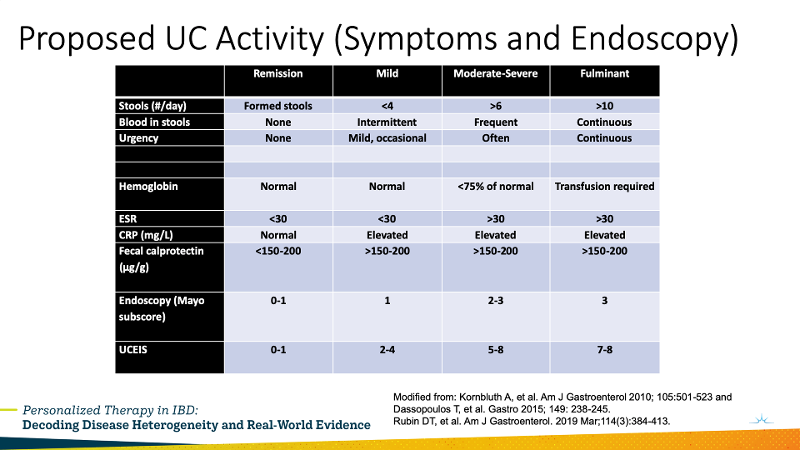
Additionally, he showed a slide adapted from the literature about current recommendations for assessing disease severity in UC.
1:40: Millie Long, MD case presentation: UC risks are onset at young age, pan-colitis, need for steroids. A patient with moderate to severe colitis, with moderate on colonoscopy between the flares she gets each fall. A young patient with years of activity of pan-colitis. This would be a good patient for a biologic. Vedolizumab was chosen with significant improvement.
Severe Perianal Disease. 2:18 Case discussion of severe perianal disease in a male. Some rectal disease. Maximize medical therapy, Push Infliximab to a level of 20. Perianal disease gets infliximab primarily. Dr. Karnbluth advocated that the surgeon needs to be an IBD experienced surgeon. Surgeons want luminal disease control first, then treat by drainage when complex, but tend to be conservative due to concern over complication risk.
2:54 Stem cells in Fistulas. There was a paper last year at DDW that used stem cell injections into perineal fistulas. This looks like it will work. It is still experimental, but with effectiveness of 50-80% it is looking good.
3:15 Malignancy with Crohn’s. When malignancy arises stop Infliximab and 6-MP. While interrupting therapy is a problem, stopping and restarting after treatment of the malignancy is generally recommended. This is mostly due to studies having excluded patients with malignancy. There is a risk of immunogenicity on restarting the infliximab.
The experts recommend that in patients on immunosuppressants go ahead and have seen by a dermatologist. This is for melanoma risk. A patient with Crohn’s was discussed, who developed a squamous cell ca. Stopping the azathioprine was suggested based on a small study showing small increase in risk of complications of the squamous cell ca. Basal cell ca doesn’t seem to be worsened by azathioprine. But the experts recommend starting a biological for 6 months before stopping the azathioprine to prevent flares.
Tofacitinib is associated with non-melanoma skin cancer.
Continue the Dermatologist screening long term even if drugs stopped.
Lymphoma: Patient developed T cell lymphoma on immunosupression therapy. Anti-TNF needs to be stopped with lymphoma. She was switched to Vedolizumab and did well. Even had a second child!
ECCO Keynote Speaker: Lessons from ECCO Thursday, December 12, 2019 from 4:15 pm to 4:45 pm Séverine Vermeire, MD University hospitals Leuven and KU Leuven university
She advocated that we check TPMT.
Optimize anti-TNF. Europeans are not recommending routine therapeutic drug monitoring. (I think this is outdated. There are studies that support it. I suspect the Europeans will change.) But in patients that lose their response doing therapeutic drug monitoring is recommended. They had a study that showed no benefit of proactive drug monitoring. That said, the speaker then described a very sophisticated use of therapeutic drug monitoring.
Keynote Speaker: Lessons Learned from Functional GI: Understanding and Treating IBS in IBD Thursday, December 12, 2019 from 5:05 pm to 5:35 pm William Chey Michigan Medicine
IBS is a heterogeneous disease that is affected by activation of the GI immune and enteric nervous system.
There is an overlap between IBS and IBD symptoms. Of IBS patients that meet Rome II criteria only 2 of 500 will have IBD. So it is very low, but not zero. However, 30-40% of IBD patients have IBS symptoms.
While we may not have a cure we have treatments that will allow patients to take back control of their lives.
He recommends an integrative approach: Diet, Followup with pharmacotherapy and stress management. Psychological treatments.
Glutamine has been effective in post infectious IBS.
Probiotics have been effective in IBS as well. The variety of probiotics is huge, but we don’t know which probiotic to use, since there are so many probiotics used, and we don’t know which one.
Leverage of microbiome or metabolome may be key.
Peppermint oil works as a smooth muscle relaxant. Uncharted peppermint oil drives GERD, so a coated preparation should be used.
5-HT3 antagonists are beneficial. Aldosterone was good but pulled. Ondansetron for IBD-D, 4-8 mg tid.
Eluxadoline available at 75 or 100 mg, don’t use in drinkers over 3 per day or after cholecystectomy. Pancreatitis and SOD dysfunction have been seen.
Rifaximin effective in multiple controlled trials. Only a 105 clinical improvement. 1/3 patients had a durable improvement. 2/3 needed longer therapy. No adverse effects seen compared to placebo.
Neuromodulators also effective. Tricyclics are not good anxiolytics, so an SSRI should be considered in that group.
Patients with Crohn’s and Colitis need their doctors when they are sick, but what should be done when they are well?
So, you have IBD, either Crohn’s disease or ulcerative colitis. Your doctor has worked with you to deal with your underlying disease. What should you do between flares of disease and long term?
Gastroenterologists think of their patients in several ways. One major way to think about our patients is what are we doing for treatment of the disease and what are we doing for general medical care. Gastroenterologists are specialists in digestive disease. But all gastroenterologists first are trained in internal medicine before getting the additional training to become a gastroenterologist.
An article in the April 2019 issue of Clinical Gastroenterology and Hepatology had a nice review of preventive care for patients with IBD. The recommendations fall into two broad categories: Screening Recommendations and Recommendations for follow up for certain drugs.
Screening Recommendations
Screenings are done to prevent certain problems that affect IBD patients more often related to risks due to the underlying disease and due to treatments.
Immunizations in IBD include the usual recommendations. Special attention is due to Influenza, pneumonia, and shingles. Flu shots with injected vaccine is recommended. The live virus nasal vaccine should be avoided. Pneumococcal vaccine should be given to all IBD patients on immunosuppression, shich is pretty much everything except mesalamine related drugs. Shingles vaccine is recommended for IBD patients over age 50. All IBD patients should get the HPV vaccine.
Skin cancer risk is increased in individuals on Anti-TNF drugs, azathioprine, 6-MP, and tofacitinib. Routine use of sunscreen and protective colthing is advised. Acute sunburn is more common on steroids as well, due to photosensitization. Consultation with a dermatologist is suggested.
Exercise is recommended for all patients to decrease the risk of osteoporosis. Calcium and Vitamin D should be checked and supplemented as appropriate. The paper says that about 1000 IU of vitamin D is needed. I believe the paper is incorrect here. Vitamin D is usually low in patients and a dose of 5000 IU of cholecalciferol is needed to keep the level over 4000 ng/dl in most patients.
Patients have an increased risk of colon cancer. Colonosocpy is recommeded in patients with over 30% of their colons involved with IBD after 8 years of disease or sooner if other family risk factors are present. If sclerosing cholangitis is present then colonoscopy should be done as soon as practicable.
Women on immunosupression should get yearly PAP smears.
Patients on steroids for more than 3 months should get a DEXA scan for checking bone mineral density. (Budesonide and rectal steroids are not as risky.)
Recommendations for follow up for certain drugs
Certain drugs need specific follow ups.
Drug
Tests
Notes
Mesalamine
CBC Creatinine UA
Allergic nephritis can develop. Check every 3-6 months.
Thiopurines
CBC LFTs
Check TPMT before starting if available to identify patients.
Methotrexate
CBC Creatinine LFTs
At start, weeks 2, 4, 8 then every 1-3 months. Give folic acid. Chest x-ray at 6-12 months.
Tofacitinib
CBC LFTs Lipid Panel TB test Hepatitis B
Check labs every 3 months. Check lipid panel at 4-6 months. Check TB test at start and 2 months into treatment. Get Hepatitis B tests before starting.
Biologics
CBC Creatinine LFTs TB test Hepatitis B
Get TB and hepatitis B tests before start. Check for TB twice a year in high risk patients. Get Hepatitis B tests before starting.
Final Thoughts
You can bring this to your doctor or send the reference to the article that I have provided below. Also, do your part and show up to see your doctor. He can’t do his part if you don’t do your’s!
References
Weaver KN1, Long MD2. Preventive Medicine in Inflammatory Bowel Disease. Clin Gastroenterol Hepatol. 2019 Apr;17(5):824-828. PMID: 30529728.
Readily available in stores and pharmacies, probiotics are a popular product that people take thinking they are good for your health. But if you buy a product you should expect it to remain unchanged over time. A recent article discusses the problem that probiotics are not regulated.
Probiotics are a polular product used by millions and big business, too. These products promise improved health, but at the same time don’t make health claims. I have a real problem with these products, because the cost my patients money but I don’t see them gettting benefit.
A major problem I see is that since they come in pill form people imagine they are like medical pills. However, each brand has different bacteria or groups of bacteria. We don’t know if probiotics work due to the surface structures on the germs or if there are metabolites that bacteria make that affect health, so it isn’t relly even known if the probiotics need to be alive or dead.
Another major problem is you don’t know what you’re getting even from time to time that you get a probiotic. It’s been known that in the growing of bacteria the bacteria can change over time. An article in by Claudio de Simone from the University of L ‘Aquila published in Clinical Gastroenterology and Hepatology(1) is worth a read as it discusses a number of points regarding the problem of probiotics not being regulated.
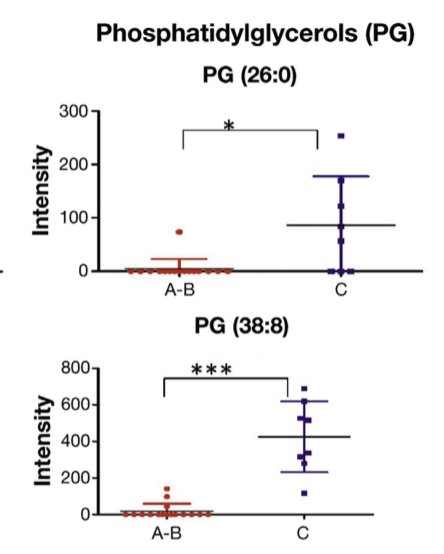
The following snippet from the article is from figure 2 in the article. Phosphatidylglycerols are an important part of bacterial cell membranes and the ratios of these are characteristic of different types of bacteria. If two bacteria are the same their PG ratios will be the same. In this example a probiotic was analyzed that was sold in the US and Italy. As can be seen, the Italian version of the probiotic had a different PG content then the US version, even though thew were sold as the same product.
One has to conclude that these products have different bacteria in them. It is a concern that may probotic products have differing bacteial content from year to year or batch to batch.
Another important point is that with many IBD patients having leaky gut that these probiotics are introducing to new bacteria in patients who could have those bacteria wander across their intestinal surface into the tissues. Given that we don’t have good safety data in IBD patients with this products and that the products also change what is in them over time I wouln’t recommend these products to patients.
References
de Simone C1. The Unregulated Probiotic Market. Clin Gastroenterol Hepatol. 2019 Apr;17(5):809-817. PMID: 29378309.
This narrative review provides an overview of the current regulation of probiotics, with a focus on those used for the dietary management of medical conditions (Medical Foods). […]
I’m new to this WordPress system. I set up the system to allow comments, but it was filled with 3000 spam articles from illegitimate online pharmacy advertisements. I’ve deleted all the comments.
I am working with my registrar/hosting serive to get this working. I still cannot register new users, and comments are still screwed up. I hope the staff at name.com will get this fixed, soon!
Readers can get access to the New England Journal of Medicine (NEJM) where 3 articles can be viewed every month. This requires a simple signup. This is such a useful tool I added a navigation page about it.
The website IBD Sucks is aptly named. It is an older site, but has a very focussed set of links related to IBD. Back in the day, it was known as the QurlyJoe site. I still don’t know what that means. Now, there are chat rooms there for support. A simple registration is needed, but get inside and lots of links!
The duration of benefit of Anti-TNF drugs for ulcerative colitis is not well understood, This article shows about 3 years of benefit on average with some UC patients getting 7 years or more of a response.
When Remicade came out it was a breakthrough in treatment for patients with Crohn’s disease. Eventually it came to be recognized as a treatment for Ulcerative Colitis as well. We went through a time of using it while on mesalamine and azathioprine, then just Remicade alone, now back to with azathioprine at low dose, and perhaps now with mesalamine again.
Aside from how to best administer anti-TNF drugs it was found that patient’s immune systems could make antibodies against them. After all, the drugs like Remicade (infliximab) and Humira (adalimumab) are themselves antibodies and therefor are proteins. The patients’ immune systems see these as foreign proteins and therefor can develop an immune reaction against them. Infliximab and adalimumab were designed to minimize immugenicity. (Immunogenicity is the word that describes no stimulating something is to the immune system). However, the immune system responds very well to foreign substances. An immune reaction often develops.
Inflammatory bowel diseases are also the result of many aspects of the immune system driving a reaction. While Tumor Necrosis Factor is one of the control proteins of the immune system it is not the only one. A patient may have multiple drivers of their disease in addition to TNF. This probably explains why only about half of patients respond to Remicade in the first place.
Once a patient responds and is on infliximab or adalimumab will it work forever? Gastroenterologists find that after a few years patients may stop responding. Tests can be done to see if antibodies are forming or if the concentration of the drug is low. But sometimes the effectiveness of anti-TNF drugs just wanes.
Crohn’s patients have been treated the longest, since the anti-TNF drugs were first used in them. We see very long duration benefits of anti-TNF drugs in many patients with Crohn’s. A number of studies have looked at the time course of response in Crohn’s disease.
Ulcerative colitis has been treated with anti-TNF drugs for a lesser number of years, so there are fewer articles obout the effectiveness of anti-TNF drugs in ulcerative colitis. An article in IBD Journal, Treatment Persistence of Infliximab versus adalimumab in Ulcerative colitis: a 16 year single-center experience[1], addresses the issue.
In this study researchers at the Nancy University Hospital in in Nancy, France reported on the results of treatment of ulcerative colitis patients that had been on long term therapy for at least 6 months. They selected patients who were treated for UC with either infliximab or adalimumab. Patients treated just for pouchitis were not included and neither were patients who had just gotten intermittent doses.
They found 160 UC patients that fit the definition of chronic use of and anti-TNF for over 6 months. In that group 43 patients had started on one of infliximab or adalimumab and swithced to the other. On average, patients responded for about 3 years (3.1 years for infliximab and 2.1 years for adamimumab. Patients that were also on mesalamine drugs had a longer duration of response.
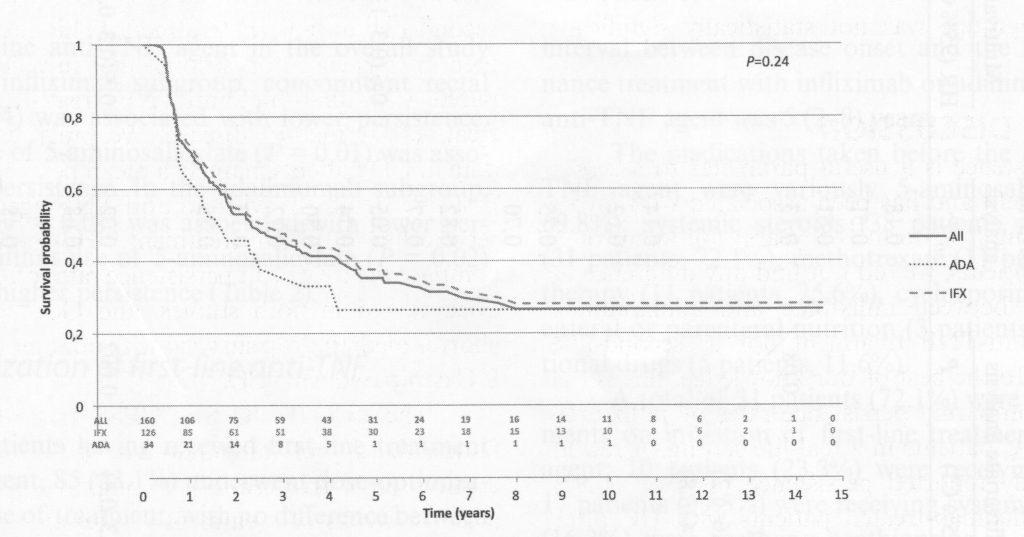
The telling graphic from the study is the analysis of time to failure of anti-TNF treatment, figure 2 in the article.
The label on the vertical axis “Survival Probability” means the proportion of patients for whom the anti-TNF drug continued to work, not time to death. The label could better have been “Proportion of patients still in remissiokn.” The number at the top is 1, meaning 100%.
Looking at the graph everyone was good for a few months, but then the drop-off is evident. While the average time of benefit was about 3 years, that includes the people with long term benefit. So for infliximab about half of individuals lost benefit at 2.3 years, and about 25% of patients had benefit that exceeded 10 years. For adalimumab, about half of individuals lost benefit at 1.7 years, but, similar to infliximab, about 25% had long term benefit.
This sort of data is very helpful in deciding on how to use anti-TNF medications. The study only looks at infliximab and adalimumab. Golimumab, certolizumab were not included, but those drugs are not as commonly used as infliximab and adalimumab in the treatment of UC.
The study is from an academic medical center, where patients are referred from the community, often sicker and less responsive than patients in the community. Thus, results may be worse than seen in community centers.
Reference: 1. Lieven Pouillon, Cédric Baumann, Hélène Rousseau, Myriam Choukour, Charlotte Andrianjafy, Silvio Danese, Laurent Peyrin-Biroulet, Treatment Persistence of Infliximab Versus Adalimumab in Ulcerative Colitis: A 16-Year Single-Center Experience, Inflammatory Bowel Diseases, Volume 25, Issue 5, May 2019, Pages 945–954, https://doi.org/10.1093/ibd/izy322
Perhaps you’re getting confused by all the medications that are now available for treating IBD. A recent article in IBD discusses the drugs by groups.
Year ago all we had to treat IBD was prednisone. Sulfasalazine ushered in the era of mesalamine drugs. Azathioprine was available as well. Then it got interesting. Our colleagues in immunology research looked into what drove the immune response and identified cachexin, also known as Tumor Necrosis Factor alpha, or TNF-α for short, as a major signaling protein in immune responses. cA2 was an antibody directed against TNF-α, which was shown to be useful in Crohn’s. Soon named Infliximab, the antibody revolutionized treatment of inflammatory bowel disease.
But our immunology colleagues have not been idle. The immune response control system has ben studied for years now, and additional targets ahve been identified in the immune system. We now have more drugs than we could have dreamed of years ago for the treatment of IBD.
A recent review [1] published in IBD Inflammatory Bowel Diseases, a journal of the Crohn’s nd Colitis foundation has provided a nice summary of some current and new drugs for use in IBD. It’s worth a read. I’m providing some highlights here.
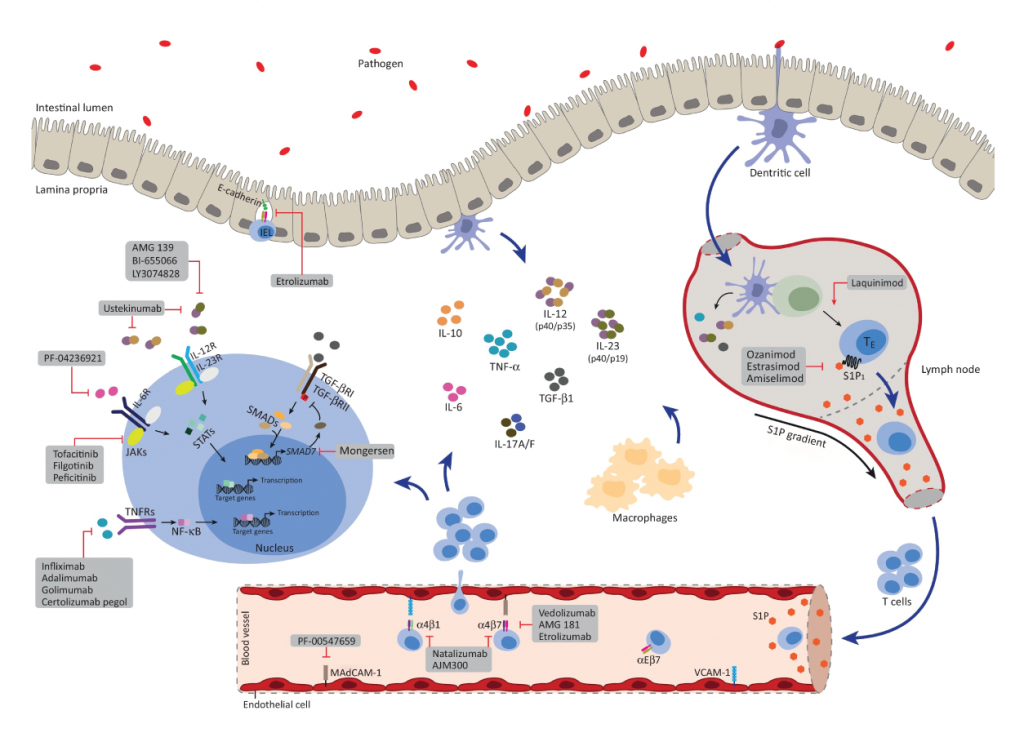
First off, the graphic on the cover of IBD is awesome. The immune system is complex, and a cartoon such as was on the cover is very helpful in putting a model in the readers head. I took this diagram off the cover of the issue of IBD. I really like the diagram. You can see that it shows a number of the molecules that are involved in the immune system of IBD.
Anti-adhesion agents
First mentioned in the review are the Anti-adhesion agents. You see, for the immune system to deliver immune cells to that are of inflammation, the cells of the immune system have to migrate to the area on inflammation. I recall stunning videos of immune cells whipping around in the vascular system, with cells stiopping in surreal instantaneity at the place they need to migrate, and then migrate through the wall of the blood vessel to the are of inflammation. If you can stop cells from finding where they need to go, the immune cells will not get to their targets and an inflammatory resposnse can be prevented. Natalizumab was the first drug in category to come to clinical practice. A protein on the surface of immune cels, α4β7/α4β1, binds to a structure named MAdCAM-1 and a structure on the inner surface of blood vessels (VCAM-1 – Vascular Cell Adhesion Molecule-1). Natalizumab is an antobody that binds to α4β7/α4β1, shich bloks cells from binding to blood vessel linings, thus preventing an immune response.
Regretably, natalizumab has been associated with the develoopment of Progressive Multifocal Leucoencephalopathy, a dangerouse disease caused by reactivation of infection by the JC virus, a not uncommon infection that the immune system usually keeps under control.
This is an example of how, even though we have a promising new drug, surprises appear when we block the immune system, allowing an infection that stays controlled by the immune system.
Vedolizumab is another anti adhesion drug. This antobody just blocks the α4β7 protein. Progressive Multifocal Leucoencephalopathy does not seem to occur with this drug. The review nicely describes the studies that support the use of Vedolizumab.
The review describes a drug under study, Etrolizumab, which is directed against the β7 molecule, so it is effective in interfering with several of the proteins that are involved with cell binding to surfaces.
AJM300 is another drug under study, but is special because it is not an antibody. It is a small molecule which blocks immune cell binding to the MAdCAM-1 and VCAM-1 proteins. This is a welcome new agent, as it can be taken as a pill rather than an injection, which is needed by antibodies. Time will tell what adverse reactions happen. Certainly, the incidence of progressive multifocal leucoencephalopathy will need to be watched for, since that problem was seen with natalizumab.
Anti-interleukin Inhibitors
Aside from TNF-α, other immune proteins are involved in the cascade of immune reactions that drive inflammatory bowel disease. IL-2, IL-12, IL-23 are all important. While prednisone blocks IL-2, the drug ustekinumab blocks IL12 and IL-20. It is effective in Crohn’s disease and psoriasis.
Risankizubmab is under development. It looks like it will also be effective in Crohn’s disease.
JAK/STAT inhibitors
In the immune system a number of chemicals are important in regulation of the immune system besides the interleukins. That is because the proteins that regulate the immune system interact with cells which then elaborate internal chemicals in response to stimulation by the interleukins. One such system is the JAK/STAT proteins. If those cellular signalling systems can be blocked then the immune system can be shut down in another way.
Tofacitinib is currently on the market, and works by blocking the JAK system. It works in Psoriasis and Ulcerative Colitis. It is a small molecule, and taken as a pill rather than an injection.
Filgotinib also blocks the JAK system, but works better in Crohn’s disease. It is currently under investigation.
Spingosine-1-phosphate receptor modulators
The review gives short shrift to this class of immun modulators, and honestly, I need to brush up on this system to tell more about what it does in the body. A drug, Ozamimodh is a small moledule orally administered It is in development and is promising for Ulcerative Colitis.
Stem Cell Therapy for perianal Crohn’s Disease
The review describes the injection of stem cells for treatment of perianal fistulas. As the review states, it isn’t known how stem cells work. These are very experimental treatments. The therapy advertised which uses cells from the stems of plants are not stem cells in the sense of stem cells from humans and have nothing to do with this.
Conclusion
This review looks over the new therapies of Anti-adhesion agents, Anti-interleukin Inhibitors, JAK/STAT inhibitors, Spingosine-1-phosphate receptor modulators, and Stem Cell Therapy. While it is written fo rthe professional, a non-professional can glean the complexity of the immune system and the exciting new options for treatment that the future protends. I’d quibble with the term Anti-interleukin Inhibitors since Anti-interleukin antibodies would be a better term. But overall the paper does describe new treatments that are available and others that will be available in the future.
I do get irritated by some things I see happening to IBD patients. There is an infectious condition called Clostridium difficile colitis which can be treated with antibiotics. One antibiotic, vancomycin, is very expensive when used in the capsule formulation, but inexpensive when supplied as a solution.
Vancomycin is a treatment for C. Difficile colitis, but can it be obtained for less than $1000?
I had a patient, recently, who is uninsured who was treated for C. difficile colitis. I was saddened to hear that she was given a prescripiton for oral vancomycin capsules. If there is one way to sour a self-pay patient on modern medicine it is to prescribe off patent medications in an expensive formulation. I have to say I learned this trick a long time ago from a coleague. I regret I don’t recall who told me, but it saves thousands of dollars.
Do I exagerate? No! Vancomycin capsules for a 10 day course of 250 mg four times a day cost upwards of $1000? So, how do you save money? Get a pharmacist to dispense the solution used for IV administration.
IV vancomycin has been available for years for about $15 for a 10 gram dose. That is just the amount needed for an oral course of therapy. Just have the pharmacist mix up the following:
Vancomycin HCl 10 g inj., 1 vial
Saccharin Sodium, 0.4 g
Stevia, 0.4 g
Glycerin, 80 ml
Raspberry concentrate, 0.2 ml
Distilled water, qs 200 ml
Sig: Take 1/2 teaspoon (2.5 ml) by mouth 4 times daily for 14 days. (2 ounces (60 ml) will be left over if nothing spilled)
This has a stability of 14 days if refrigerated. She has Crohn’s disease and has recurrent C. diff which I found upon scoping her, today. This script will cost about $50-$80, saving her about $900 to $1000. She thinks I’m great for having found this cheaper alternative. Next step may be a stool transplant (which might cure her Crohn’s!).
I originally found this recipe for compounding Vancomycin at the American Society of Health-System Pharmacists web site. The link went dead so I subbed in the content from the Internet Archive. The internet is a wonderful place, and Google serves us well. The recent script I wrote left out the Stevia, and just ordered “flavor, prn”, leaving that to the judgement of the pharmacist. Don’t fear writing a compounding prescription. Pharmacists are our friends, and they like the chance to provide this service to our patients.
Links fixed, made prescription easier to copy and paste – 10/20/22